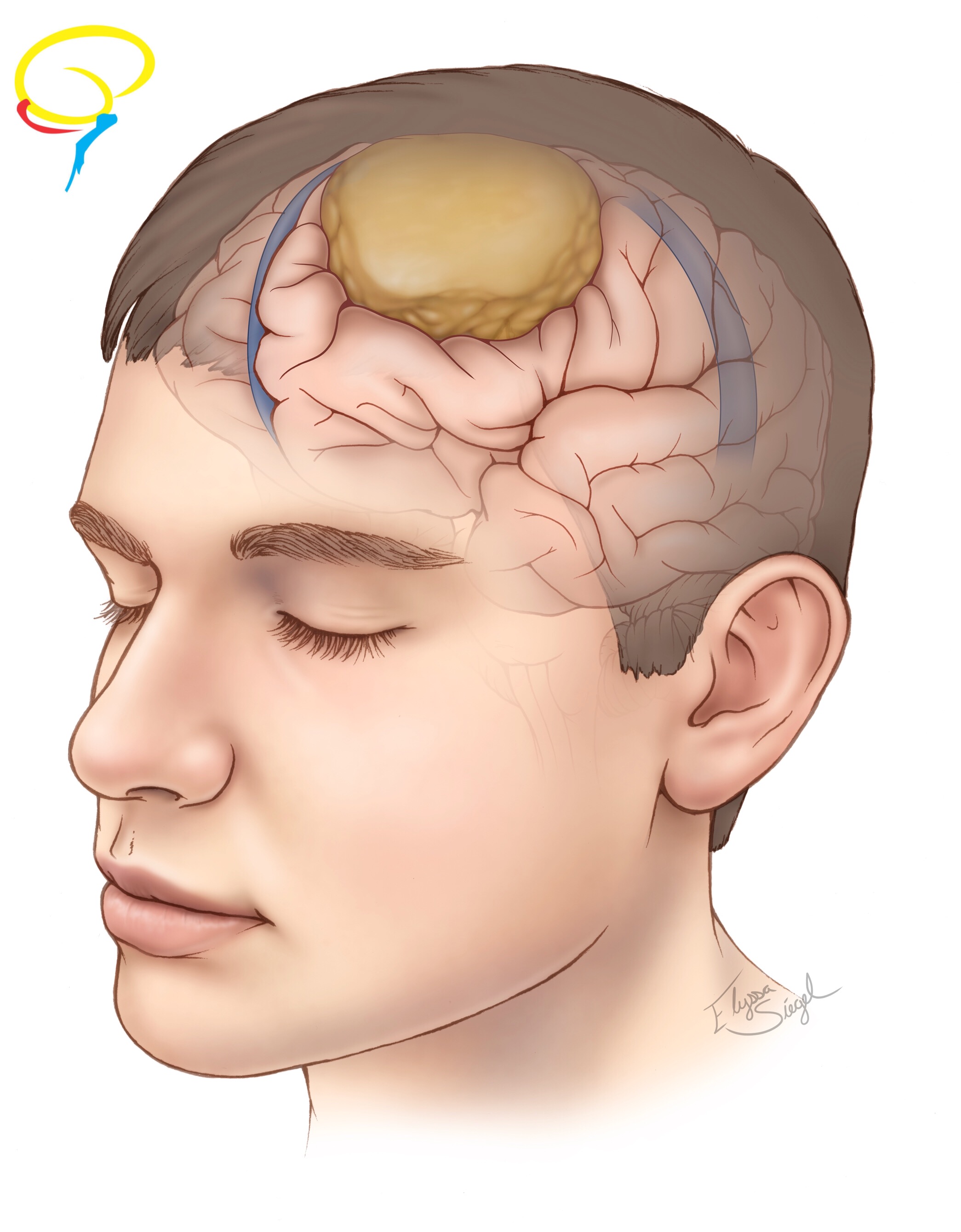
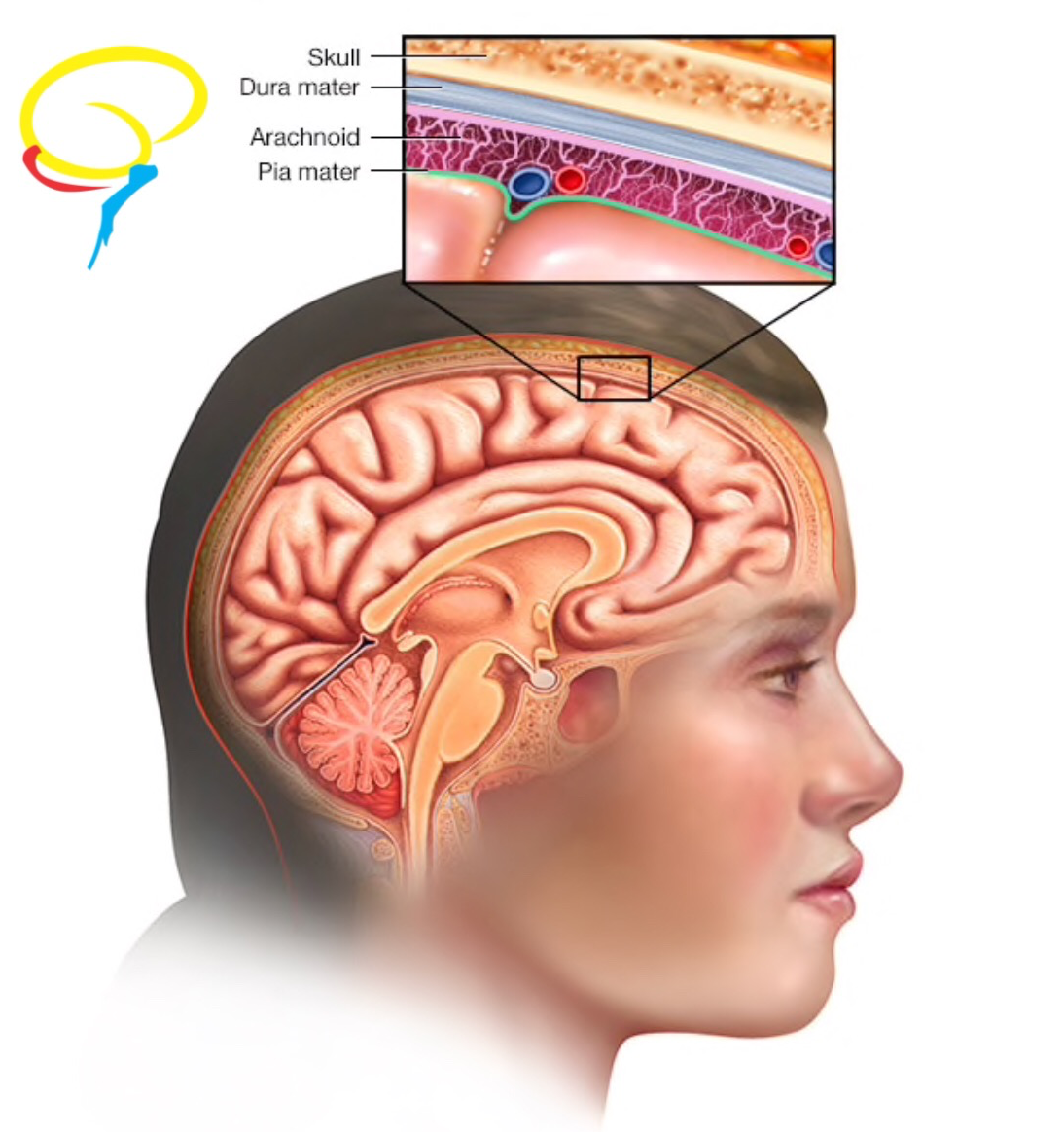
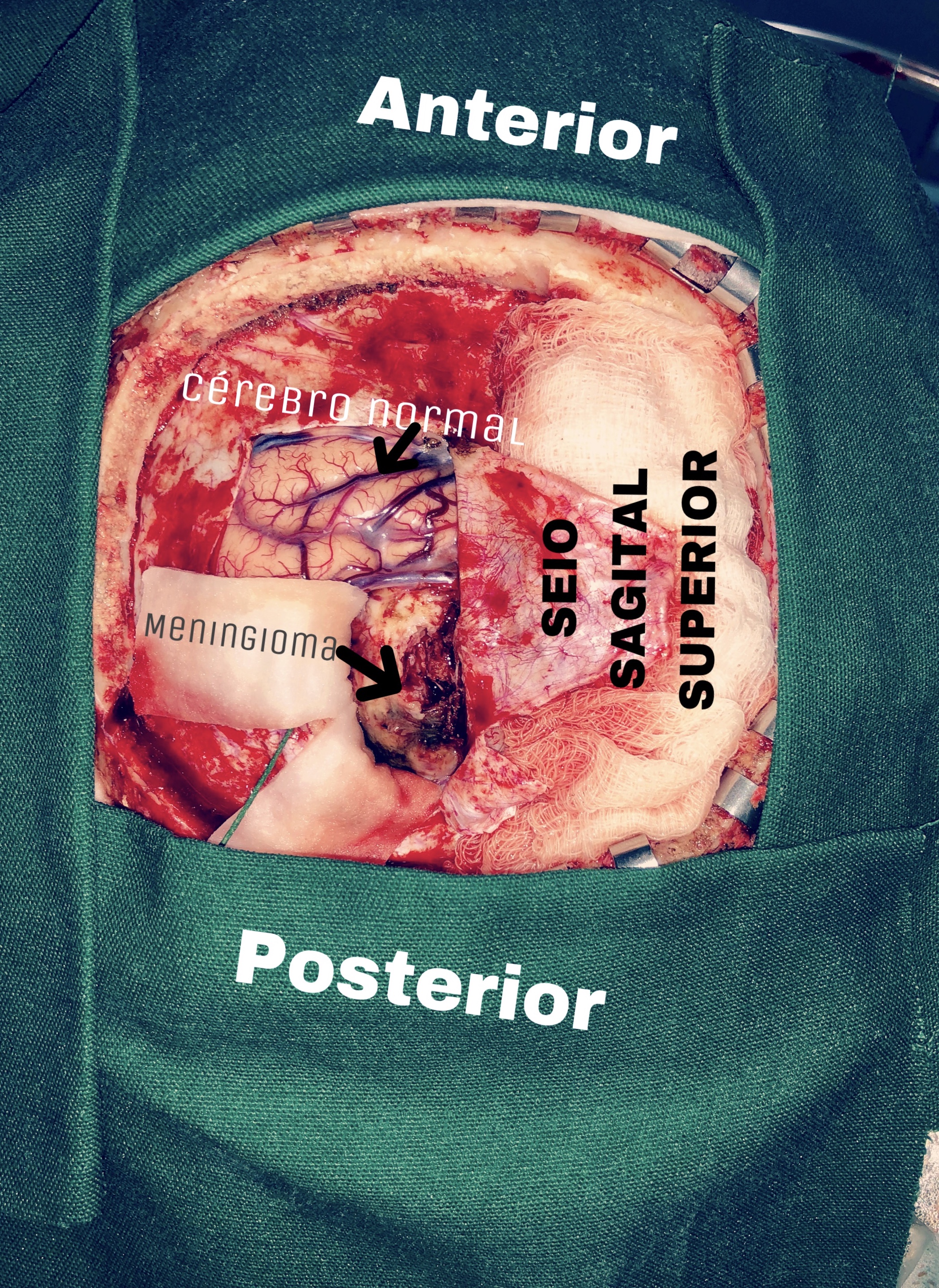
Meningiomas are benign tumors that grow from the meninges (the protective membranes that cover the brain and spinal cord), or, more specifically, from the arachnoid cells (Figures 1 and 2). They are more frequently found in women between the ages of 40 and 60 year. They are mainly located under the cerebral convexities, near the venous sinus, along the base of the skull, in the posterior fossa and rarely within the ventricles. There may be multiple meningiomas. Meningiomas compress, but do not invade the cerebral parenchyma. They can invade and distort the adjacent bone. There are several histological types, which may influence in the clinic evolution and some become malignant (Figure 8).
It is known that meningiomas may arise from radiotherapy of the central nervous system, but radio-induced cases are rare and only high doses of radiation could cause a tumor. Hormonal influence in meningiomas is not a well-established risk factor yet. Family medical history is also rare e is related to genetic syndromes, like Neurofibromatosis.
The symptoms depend on what part of the brain is compressed, and therefore, on the location of the tumor.
| Meningioma symptoms, according to location | |
| Location | Symptoms |
| Base of the skull | Visual loss
Oculomotor nerve palsy Exophthalmos |
| Cerebral convexities | Focal epileptic seizures
Cognitive deficits Finally, signs of increased intracranial pressure |
| Clivo and apical petrous bone | Gait abnormalities
Limb ataxia Deficits in the V, VII, and VIII cranial nerves |
| Foramen magnum | Ipsilateral suboccipital pain
Paresis, starting in the ipsilateral arm, evolves into the ipsilateral leg and then to the contralateral leg and arm Sometimes, Lhermitte’s Sign Cranial nerves deficits (e.g. dysphagia, dysarthria, nystagmus, diplopia, facial hypoesthesia) |
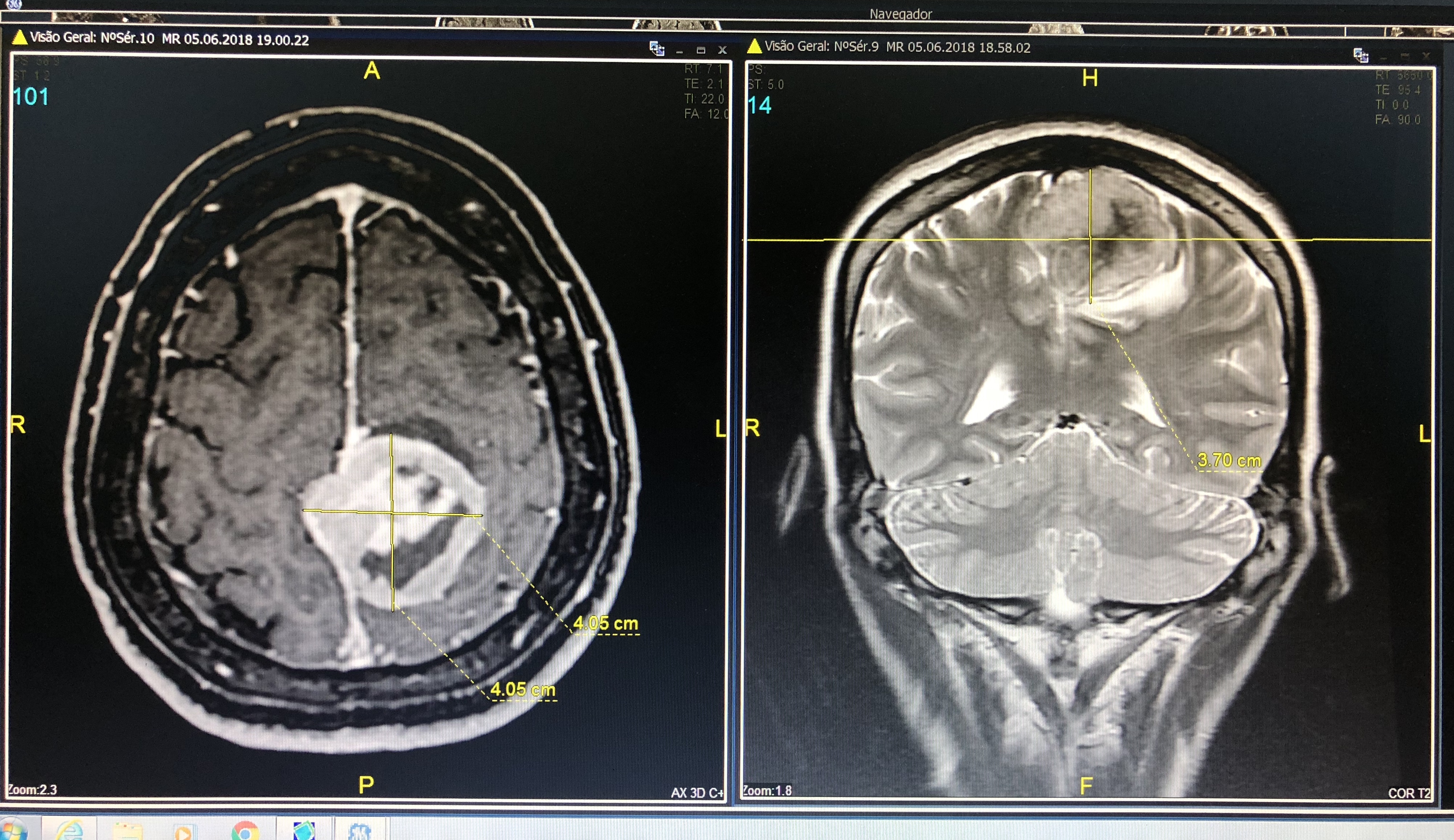
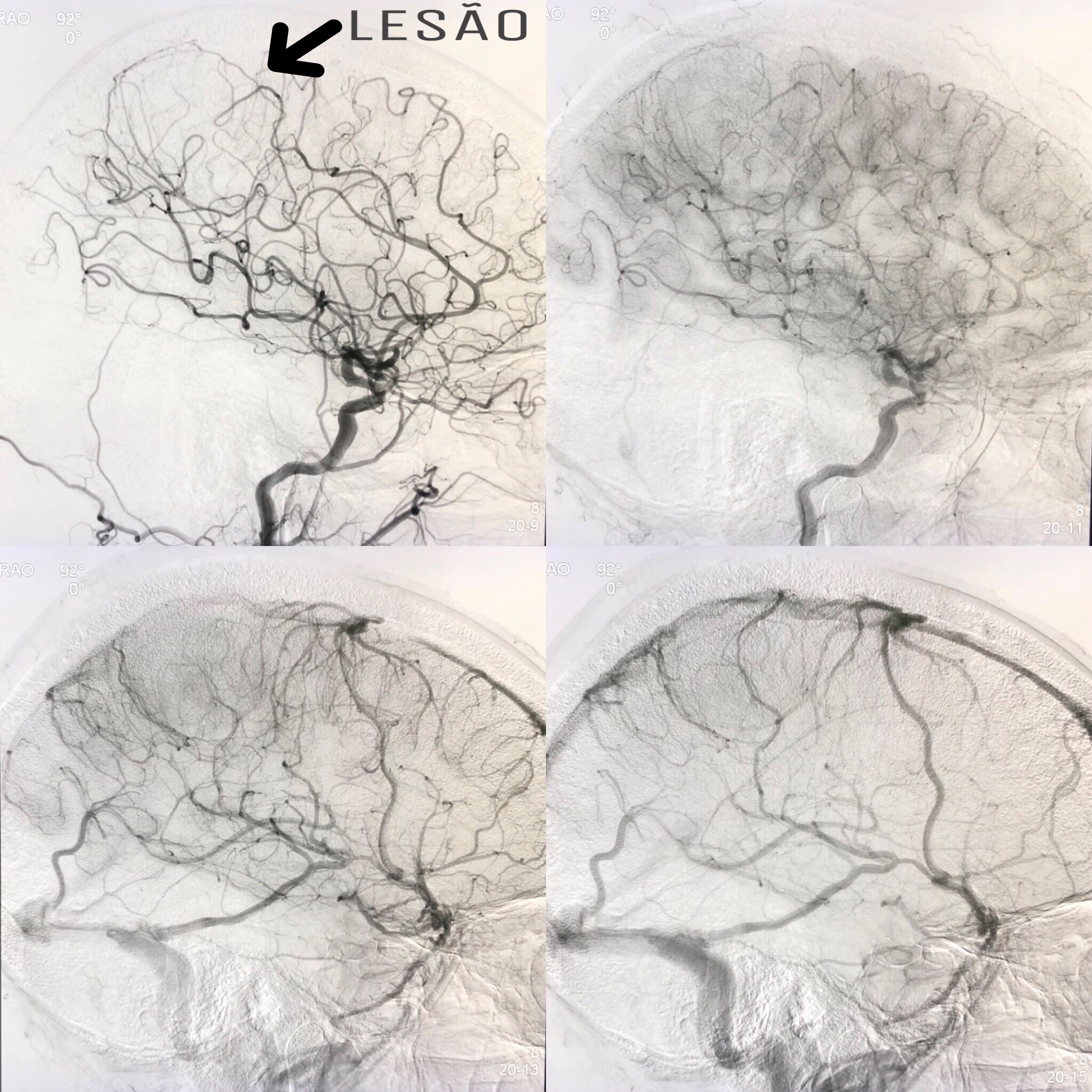
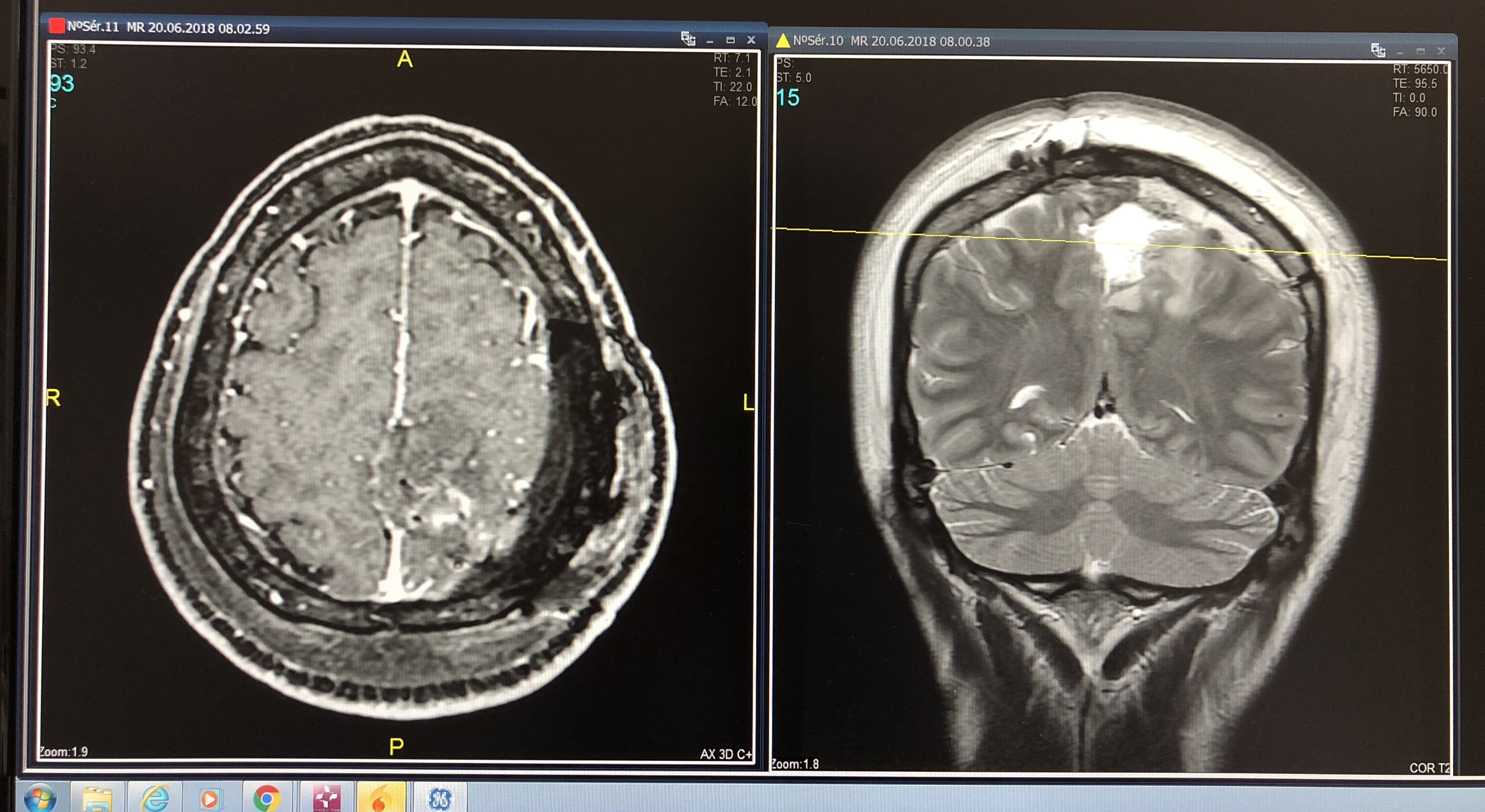
To diagnose a meningioma, a neurologist will conduct an imaging test, such as magnetic resonance imaging, of the brain (Figure 3). Cerebral angiography can help in the treatment strategy, by assessing the arterial nutrition of the tumor and venous sinus obstruction (Figure 4). If the case allows, preoperative embolization can be performed in order to reduce the tumor blood supply, minimizing intraoperative bleeding and facilitating surgery.
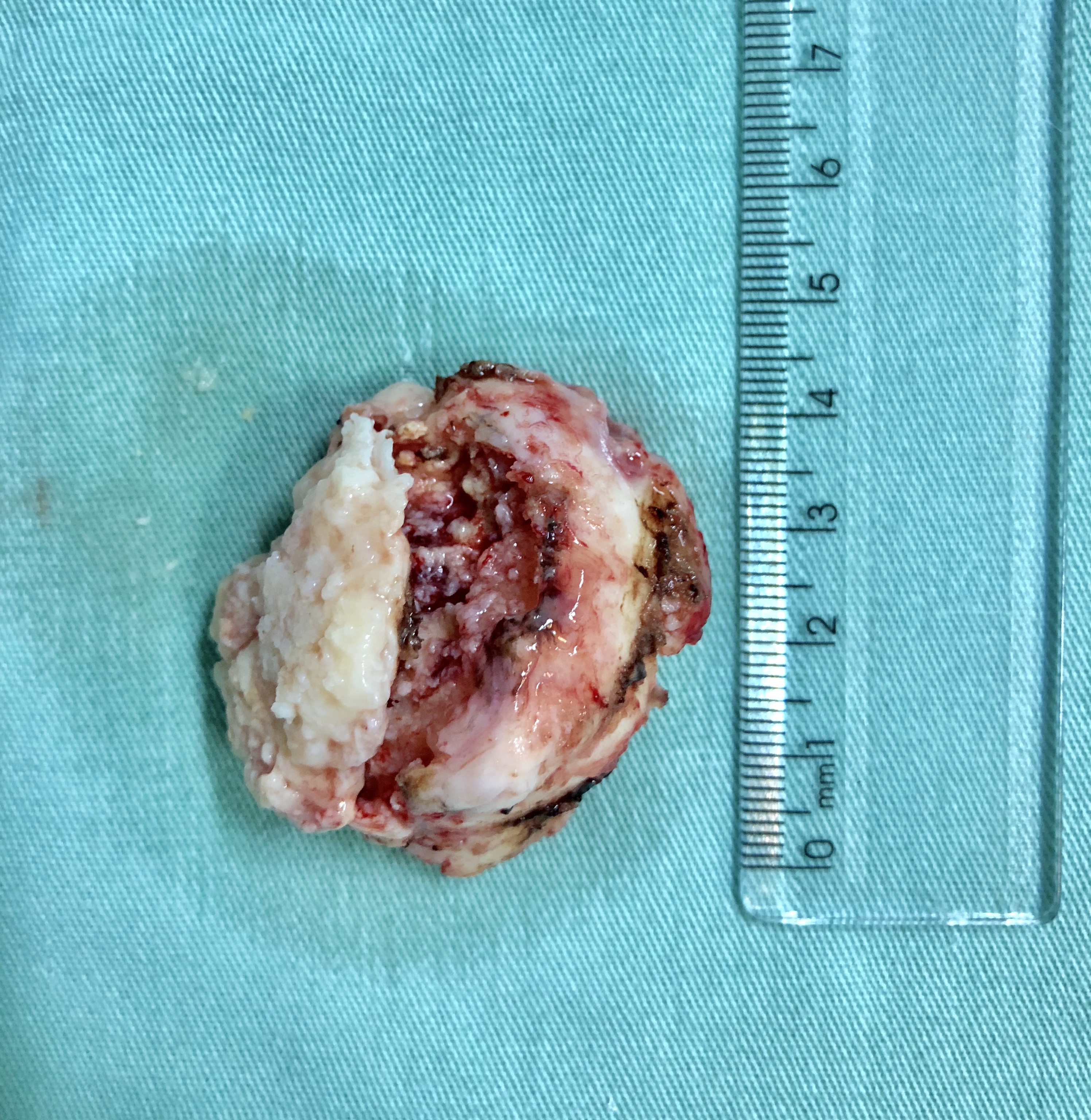
Surgery is the most effective treatment for this type of tumor and it is usually possible to remove it completely and cure the disease (Figures 5 and 6). Sometimes, surgical removal can be difficult due to the complex surgical access, as in cases of petro-clivial, spheno-orbital, cavernous sinus or the dural venous sinus meningiomas, as in the case presented. In this situation, other treatments like radiotherapy and radiosurgery can be performed.